马上注册,结交更多好友,享用更多功能,让你轻松玩转社区。
您需要 登录 才可以下载或查看,没有账号?立即注册
x
TBD |
|
|
|
|
|
|
共3条精彩回复,最后回复于 2015-5-14 12:19

尚未签到
Pembrolizumab (pembro; MK-3475) plus platinum doublet chemotherapy (PDC) as front-line therapy for advanced non-small cell lung cancer (NSCLC): KEYNOTE-021 Cohorts A and C.
Pembrolizumab联合铂类双药化疗作为晚期NSCLC的一线治疗效果研究:KEYNOTE-021 队列A和队列C
Abstract:
Background: As monotherapy, the anti–PD-1 antibody pembro has shown robust antitumor activity in advanced NSCLC patients (pts). KEYNOTE-021 evaluated the safety, tolerability, and clinical activity of pembro + PDC for treatment-naive advanced NSCLC.
背景: anti-PD-1抗体pembro作为单药在晚期NSCLC患者中表现出强烈的抗肿瘤活性。KEYNOTE-021临床验证了pembro联合铂类双药在未接受治疗的晚期NSCLC患者中的安全性、耐受性和临床疗效
Methods: Pts with stage IIIB/IV NSCLC and no prior systemic therapy were randomized 1:1 to pembro 2 or 10 mg/kg Q3W plus carboplatin AUC 6 + paclitaxel 200 mg/m2 (cohort A; any histology) or carboplatin AUC 5 + pemetrexed 500 mg/m2 (cohort C; nonsquamous without EGFR sensitizing mutation or ALK translocation only). Pts received pembro + PDC for 4 cycles followed by pembro maintenance in A and pembro + pemetrexed in C. The dose-limiting toxicity (DLT) observation window was the first 3 wk after initial dosing. Key eligibility criteria included ECOG PS 0-1, measurable disease, and adequate tumor sample for PD-L1 assessment. Response was assessed every 6 wk until confirmed progression (RECIST v1.1, investigator review).
方法: 未接受治疗的IIIB期或者IV期NSCLC患者按照1:1的比例被随机分配到:队列A(任何组织学种类,pembro 2mg/kg或者10mg/kg Q3W + 卡铂AUC6 + 紫杉醇200mg/m2)和队列C(组织学为不具有EGFR敏感突变的非鳞癌患者,pembro 2mg/kg或者10mg/kg Q3W + 卡铂 AUC 5 + 培美曲塞500mg/m2)。患者接受pembro+铂类双药治疗4周期后,以pembro(队列A)或者pembro+培美(队列C)作维持治疗。DLT观察窗口为初始治疗后的3周。重要的入组条件包括PS 0-1,可测量病灶以及足够的用于PD-L1评估的肿瘤样本。每六周评估治疗效果直至疾病进展。
Results: As of Dec 2014, 44 pts (20 in cohort A and 24 in cohort C) were treated. One DLT was reported (hospitalization for gr 3 rash, C [pembro 10 mg/kg]). Gr 3-4 treatment-related AE rate was 27% (15% in A, 38% in C); AEs were reversible transaminase elevation (n = 3 in C), anemia (n = 1 in A, 2 in C), rash (n = 1 in A, 1 in C), and colitis (n = 2 in C); no gr 3-4 febrile neutropenia was observed. One patient in C discontinued due to treatment-related gr 3 rash. No treatment-related deaths have occurred. Preliminary ORR (confirmed and unconfirmed) is 30% in A and 58% in C (Table). At the time of analysis, 16 pts in A and 21 pts in C remained on treatment.
结果: 截止2014年12月,44位患者(队列A 20位,队列C 24位)接收治疗。一例DLT被报告(需要住院治疗的3级皮疹, 队列C)。3-4级治疗相关的AE发生率为27%(队列A 15%,队列C 38%)。AE包括可逆的转氨酶升高、贫血、皮疹和结肠炎。未观察到3-4级的中心粒细胞减少。队列C中有1位患者因为发生3级皮疹而中断治疗。有非治疗相关的死亡病例。初步的ORR为队列A 30%和队列C 58%。截止目前,队列A中16位患者和队列C中21位患者仍在继续接受治疗。
Conclusions: These data suggest that pembro + PDC has a reasonable safety profile and provides antitumor activity as front-line therapy for stage IIIB/IV NSCLC. Based on the promising ORR observed for pembro + carboplatin and pemetrexed, this combination is being evaluated in a larger cohort. Clinical trial information: NCT02039674 |
|
|
|
|
|
|
尚未签到
Phase 1 study of pembrolizumab (pembro; MK-3475) plus ipilimumab (IPI) as second-line therapy for advanced non-small cell lung cancer (NSCLC): KEYNOTE-021 cohort D.
Background: Pembro is a potent anti–PD-1 monoclonal antibody. IPI, an anti–CTLA-4 antibody, has shown activity in advanced NSCLC. In melanoma, combined anti–PD-1 and anti–CTLA-4 treatment has shown robust efficacy and manageable toxicity. We report interim results from a phase 1 study evaluating pembro + IPI in patients (pts) with recurrent NSCLC.
Methods: Pts with stage IIIB/IV NSCLC that recurred after ≤ 2 prior regimens received pembro + IPI every 3 wk for 4 cycles followed by maintenance pembro. Based on emerging data from the nivolumab + IPI advanced NSCLC study, doses were reduced from 10 mg/kg to 2 mg/kg for pembro and from 3 mg/kg to 1 mg/kg for IPI). Primary end point was safety and incidence of dose-limiting toxicities (DLTs) in the first 3 wk of dosing. Response was assessed every 6 wk per RECIST 1.1 by investigator review.
Results: As of Dec 2014,17 pts were enrolled: 3 at pembro 10 mg/kg + IPI 3 mg/kg, 3 at pembro 10 mg/kg + IPI 1 mg/kg, and 11 at pembro 2 mg/kg + IPI 1 mg/kg. No DLTs or dose modifications were reported for the 15 pts treated at the time of analysis. 10 pts experienced drug-related AEs (DRAEs); none led to discontinuation or death. There were 2 gr 3 DRAEs, both rash. Gr 2 DRAEs were diarrhea and vomiting (n = 2 each) and chills, cough, decreased appetite, decreased weight, dehydration, depression, dysphonia, fatigue, myalgia, pruritus, and pyrexia (n = 1 each). Responses were seen in all dose groups among the 11 pts on treatment for ≥ 6 wk at the time of analysis, including 1 CR (9%) and 5 PRs (45%) (Table); all pts achieved disease control. 12 pts remain on treatment (range, 6 + to 26 + wk); 3 pts discontinued for PD.
Conclusions: Preliminary data from KEYNOTE-021 cohort D demonstrate an acceptable toxicity profile and robust antitumor activity for pembro + IPI in pts with recurrent NSCLC.The use of lower pembro and IPI doses did not appear to negatively impact efficacy. Clinical trial information: NCT02039674 |
|
|
|
|
|
|
尚未签到
Phase 3 KEYNOTE-042 trial of pembrolizumab (MK-3475) versus platinum doublet chemotherapy in treatment-naive patients (pts) with PD-L1–positive advanced non-small cell lung cancer (NSCLC).
Background: Tumors can evade an immune response by co-opting the PD-1 pathway. The anti–PD-1 monoclonal antibody pembrolizumab has demonstrated promising efficacy and acceptable safety across doses and schedules in pts with NSCLC enrolled in the phase 1 KEYNOTE-001 trial, with greater efficacy observed in pts with PD-L1+ tumors. In 45 treatment-naive, PD-L1+ pts (n = 42 evaluable by RECIST v1.1 per central review), pembrolizumab provided a 26% ORR and 64% DCR. All 11 responses were ongoing after a median follow-up of 36 wk. The randomized, open-label phase 3 KEYNOTE-042 trial (ClinicalTrials.gov, NCT02220894) will evaluate the efficacy and safety of pembrolizumab vs platinum doublet chemotherapy as first-line therapy for PD-L1+ advanced NSCLC.
Methods: Eligible pts with advanced PD-L1+ NSCLC without EGFR sensitizing mutations or ALK translocation and ≥1 measurable lesion will be randomized 1:1 to pembrolizumab 200 mg every 3 wk or investigator's choice of carboplatin plus paclitaxel or carboplatin plus pemetrexed. Randomization will be stratified by ECOG PS (0 vs 1), histology (squamous vs nonsquamous), region (East Asia vs non-East Asia), and PD-L1 expression (strong vs weak [staining in ≥50% vs 1-49% of tumor cells assessed by immunohistochemistry with the 22C3 antibody]). Pembrolizumab will be continued for 35 cycles or until disease progression, intolerable toxicity, or investigator decision; discontinuation is allowed for pts with complete response. Chemotherapy will be given for a maximum of 6 cycles. Pemetrexed maintenance is optional for pts with nonsquamous NSCLC. In both treatment arms, eligible pts may be treated beyond initial radiographic progression. AEs will be collected during and for 30 d after treatment. Response will be assessed every 9 wk per RECIST 1.1 by central review. Survival follow-up will occur every 2 mo. Primary end point is OS in pts with PD-L1–strongly-positive tumors; secondary end points include PFS in strongly positive pts and PFS and OS in all pts. Enrollment began in Nov 2014 and will continue in 28 countries in Asia, Canada, Europe, and South America until the target of 1240 pts is achieved. Clinical trial information: NCT02220894 |
|
|
|
|
|
|
 求助
[attachimg]93413[attachimg]麻烦问下 rb1突变导致 最近三个月cea都缓慢增高,,只能
求助
[attachimg]93413[attachimg]麻烦问下 rb1突变导致 最近三个月cea都缓慢增高,,只能
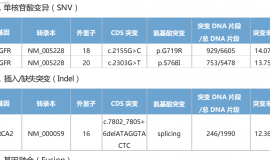
 各位大神朋友,基因检测如图所示,靶
家里老人是肺浸润性腺癌,基因检测如图片所示,想问问大神朋友,有没有遇到类似情况,
各位大神朋友,基因检测如图所示,靶
家里老人是肺浸润性腺癌,基因检测如图片所示,想问问大神朋友,有没有遇到类似情况,
 一文盘点肺癌领域ADC,看看“魔法子
作者:雨过天晴
ADC全称抗体-药物偶联物(antibody-drug conjugate)。作为一种新型抗
一文盘点肺癌领域ADC,看看“魔法子
作者:雨过天晴
ADC全称抗体-药物偶联物(antibody-drug conjugate)。作为一种新型抗
 电场治疗癌症业余实现(睡眠专用型)
便携式的肿瘤电场治疗装置已在去年本人所发的帖子中详细描述过了,居然有十多万的阅
电场治疗癌症业余实现(睡眠专用型)
便携式的肿瘤电场治疗装置已在去年本人所发的帖子中详细描述过了,居然有十多万的阅
 用药9个月肿瘤消失,抗肺癌迈向第6年
讲述者:大浩整理者:pear
2019年确诊肺癌时,我已经出现骨转移、脑转移, 医生说我“
用药9个月肿瘤消失,抗肺癌迈向第6年
讲述者:大浩整理者:pear
2019年确诊肺癌时,我已经出现骨转移、脑转移, 医生说我“



 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡