4393 The Combination Of Palbociclib Plus Bortezomib Is Safe and Active In Patients With Previously Treated Mantle Cell Lymphoma: Final Results Of a Phase I Trial
Program: Oral and Poster Abstracts
Session: 624. Lymphoma: Therapy with Biologic Agents, excluding Pre-Clinical Models: Poster III
Monday, December 9, 2013, 6:00 PM-8:00 PM
Hall G (Ernest N. Morial Convention Center)
Peter Martin, MD1, Maurizio DiLiberto, PhD2*, Christopher E Mason, PhD3*, Scott A Ely, M.D.4, Jia Ruan, MD, PhD5, Richard R. Furman, MD2, David Chiron, PhD6*, Xiangao Huang, PhD6, David C Madoff, M.D.7*, Jonathan Navi7*, Jessica Lewis, PA-C8*, Alison Bender, PA-C8*, Amelyn Rodriguez, RN8*, June Greenberg, RN9*, Morton Coleman, MD1*, Selina Chen-Kiang, PhD6 and John P. Leonard, M.D.10
1Hematology and Oncology, Weill Cornell Medical College, New York, NY
2Weill Cornell Medical College, New York, NY
3Department of Physiology and Biophysics and Institute for Computation Biomedicine, Weill Cornell Medical College, New York, NY
4Department of Pathology and Laboratory Medicine, Weill-Cornell Medical College, New York, NY
5Division of Hematology/Medical Oncology, Weill Cornell Medical College, New York, NY
6Department of Pathology and Laboratory Medicine, Weill Cornell Medical College, New York, NY
7Weill Cornell Medical College, New York
8Department of Medicine, Division of Hematology-Oncology, Weill Cornell Medical College, New York, NY
9Division of Hematology and Oncology, Weill Cornell Medical College, New York, NY
10Weill Medical College of Cornell University, New York, NY
Introduction
Mantle cell lymphoma (MCL) is characterized by cell cycle dysregulation due to cyclin D1 and CDK4 overexpression. Palbociclib (PD 0332991) is an orally bioavailable, specific, reversible inhibitor of CDK4/6 that induces prolonged early G1 arrest (pG1) in MCL cells and durable remissions in patients with MCL. Moreover, we have evidence that palbociclib-induced pG1 sensitizes MCL cells to killing by bortezomib and that sensitization is amplified upon withdrawal of palbociclib, when MCL cells synchronously enter S phase (pG1-S). Targeting CDK4 in combination with bortezomib, therefore, is a rational and novel therapeutic combination. We report the final results of a phase I trial of palbociclib plus bortezomib in patients with previously treated MCL.
Methods
Adults with previously treated MCL and adequate bone marrow and organ function were received palbociclib orally at doses of 75 mg (dose level 1), 100 mg (dose level 2), or 125 mg (dose levels 3 and 4) for 12 days. Bortezomib was administered by IV or SC injection at 1 mg/m2 (dose levels 1-3) or 1.3 mg/m2 (dose level 4) on days 8, 11, 15, and 18 of each 21-day cycle. Subjects underwent core needle biopsies of tumor tissue pre-treatment, on day 8 (in pG1) and on day 21 (in pG1-S phase) of cycle 1. Subjects were restaged following cycles 2, 5, and 8 and then every 4 cycles. Subjects could remain on the study regimen until progression, unacceptable toxicity, or withdrawal. Dose levels were escalated according to the standard 3+3 schema. Dose limiting toxicity (DLT) was defined as treatment-related grade 3-4 toxicity occurring during cycle 1 or a delay in cycle 2 of > 1 week due to treatment-related grade 4 neutropenia or thrombocytopenia. The primary objective was to estimate the maximum tolerated dose of the combination. Secondary objectives included response rate, duration of response, and evaluation of the pharmacokinetic and pharmacodynamic profiles at multiple time points and across all dose levels.
Results
Nineteen subjects were enrolled: 6 in dose level 1, 3 in dose level 2, 7 in dose level 3, and 3 in dose level 4. The median age was 64 years (range 42-81). The median number of prior therapies was 3 (range 1-7). The number of subjects with low, intermediate, and high-risk MIPI scores was 6, 11, and 2, respectively. Two subjects experienced DLT: thrombocytopenia (level 1), neutropenia (level 3). Grade 3-4 hematologic toxicity included neutropenia (63%), thrombocytopenia (53%), lymphopenia (32%), and anemia (11%). Treatment-related grade 3-4 non-hematologic toxicity included zoster (1). Grade 1-2 toxicities occurring in >2 pt included: fatigue (47%), pain (42%), bleeding/bruising (37%), increased creatinine (26%), constipation (26%), rash (21%), nausea/vomiting (21%), sensory neuropathy (21%), dyspnea (21%), hypoalbuminemia (16%), cough (16%), edema (16%), infection (16%), increased AST (16%), hypocalcemia (16%), increased alk phos (16%). Reasons for ultimately stopping treatment include: progression (9), toxicity (6), and non-compliance (1). All 3 patients at dose level 4 required dose delays/reductions during cycle 2 due to toxicity. There appeared to be an association with dose of palbociclib and response, with one responder at each of dose levels 1 and 2, and 4 patients remaining free from progression for 1 year at dose level 3, including one complete response. Only one responding patient progressed on therapy. All patients with serial biopsies achieved pG1 on day 8, with reduction in CDK4/CDK6-specific Rb phosphorylation and Ki67 by immunohistochemistry. The primary MCL tumor cells express cell cycle genes scheduled for early G1 such as cyclin D1 and CDK4, but not genes programmed for other phases of the cell cycle such MKi67, E3F3, CDK1, CCNA2, as determined by RNA-seq.
Conclusion
Daily palbociclib 125 mg for 12 days can be safely combined with bortezomib 1 mg/m2 twice weekly, while higher doses were limited by myelosuppression. The combination induced durable responses in some patients. Palbociclib induced pG1, even at the lowest dose. However, the initial cell cycle control by palbociclib did not predict clinical response. Rather, pG1 appears to induce an imbalance in gene expression that is associated with response to the combination of palbociclib plus bortezomib. Strategies to control the cell cycle and dissect the underpinning mechanisms appear promising in MCL and warrant further evaluation.
Disclosures: Martin: Teva: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Genentech: Speakers Bureau; Millennium: Research Funding; Seattle Genetics: Consultancy, Speakers Bureau. Ruan: Celgene: Consultancy, Membership on an entity’s Board of Directors or advisory committees, Research Funding; Seattle Genetics, Inc.: Membership on an entity’s Board of Directors or advisory committees. Leonard: Millennium: Consultancy. |
 求助
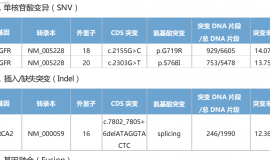
[attachimg]93413[attachimg]麻烦问下 rb1突变导致 最近三个月cea都缓慢增高,,只能
求助
[attachimg]93413[attachimg]麻烦问下 rb1突变导致 最近三个月cea都缓慢增高,,只能
 各位大神朋友,基因检测如图所示,靶
家里老人是肺浸润性腺癌,基因检测如图片所示,想问问大神朋友,有没有遇到类似情况,
各位大神朋友,基因检测如图所示,靶
家里老人是肺浸润性腺癌,基因检测如图片所示,想问问大神朋友,有没有遇到类似情况,
 一文盘点肺癌领域ADC,看看“魔法子
作者:雨过天晴
ADC全称抗体-药物偶联物(antibody-drug conjugate)。作为一种新型抗
一文盘点肺癌领域ADC,看看“魔法子
作者:雨过天晴
ADC全称抗体-药物偶联物(antibody-drug conjugate)。作为一种新型抗
 电场治疗癌症业余实现(睡眠专用型)
便携式的肿瘤电场治疗装置已在去年本人所发的帖子中详细描述过了,居然有十多万的阅
电场治疗癌症业余实现(睡眠专用型)
便携式的肿瘤电场治疗装置已在去年本人所发的帖子中详细描述过了,居然有十多万的阅
 用药9个月肿瘤消失,抗肺癌迈向第6年
讲述者:大浩整理者:pear
2019年确诊肺癌时,我已经出现骨转移、脑转移, 医生说我“
用药9个月肿瘤消失,抗肺癌迈向第6年
讲述者:大浩整理者:pear
2019年确诊肺癌时,我已经出现骨转移、脑转移, 医生说我“




 提升卡
提升卡 置顶卡
置顶卡 沉默卡
沉默卡 喧嚣卡
喧嚣卡 变色卡
变色卡 千斤顶
千斤顶 显身卡
显身卡